
The Official 2/26 Battalion Website
In affiliation with the 2/26 Battalion Family & Friends Association Inc.
-
 This is an image title
This is an image title
Lorem pellentesque habitant morbi tristique.
Estibulum erat wisi, condimentum, commodo
ornare sit wisi. Aenean fermentum, elit eget
tinciduntcondimentum.Vestibulum erat wisi
condimentum sed, commodo vitae, ornare
sit amet, wisi. Aenean fermentum, elit eget
tincidunt condimentum. -
 This is an image title
This is an image title
Lorem pellentesque habitant morbi tristique.
Estibulum erat wisi, condimentum, commodo
ornare sit wisi. Aenean fermentum, elit eget
tinciduntcondimentum.Vestibulum erat wisi
condimentum sed, commodo vitae, ornare
sit amet, wisi. Aenean fermentum, elit eget
tincidunt condimentum. -
 This is an image title
This is an image title
Lorem pellentesque habitant morbi tristique.
Estibulum erat wisi, condimentum, commodo
ornare sit wisi. Aenean fermentum, elit eget
tinciduntcondimentum.Vestibulum erat wisi
condimentum sed, commodo vitae, ornare
sit amet, wisi. Aenean fermentum, elit eget
tincidunt condimentum.
Tambaya Hospital
The following account is an actual medical report written by Tanbaya Hospital's O.C., Major Bruce Hunt depicting the atrocious conditions in which the Imperial Japanese Army (I.J.A) treated their sick and injured P.O.W'S and which he had to run a fully operational Hospital under.
TANBAYA HOSPITAL BURMA
MEDICAL REPORT AUG 1ST - NOV 24TH 1943
INTRODUCTORY.
The I. J. A. first intimated (on 29 June) that it was intended to
establish a hospital in Burma to receive men of "F" Force who would be
incapable of work for at least 2 months. Rolls were prepared for a
hospital of 2,000, but on 8 July all plans were cancelled. Fresh orders
were issued on 21 July to prepare rolls, this time for a 1,250 bed
hospital. Lt. Col. Harris, Commanding "F" Force, had appointed me O. C.
Hospital on 1 July, and on 24 July I was taken to Burma by the I. J. A.
in company with Lieut. SAITO, to examine the hospital site. I returned
on 28 July, and on 30 July the advance party left for Burma.
GENERAL COMMENT.
When the proposal for a Hospital Camp was first mooted hopes ran
high that this would be the means of saving hundreds of lives. This was
particularly the case amongst hospital patients who be reason of their
illnesses might be regarded as eligible for selection for Burma. There
seemed reasonable grounds for this enthusiasm as the I. J. A. had given
assurances that no work would be demanded from the camp and that the
dietary would be a good better than it was in the working camps; a
further statement had been made that necessary drugs and medicines would
probably be supplied.
The records contained in the War Diary indicate
that the hopes at first extended for the success of the camp were not
realised. A death rate of 660 (with a possibility of 90 - 100 more) out
of a total camp entry of 1,924 is a profoundly disappointing result. The
reasons for this high death rate are set out below. It is a melancholy
reflection that in November there was as much enthusiasm to leave Burma
as there had been in July to go there.
FACTORS CONCERNED IN THE HIGH DEATH RATE.
1. STATE OF DISEASES.
Very many patients were
in such an advanced state of disease that on arrival to Burma that even
with the best hospital facilities in the world recovery would have been
impossible. This applied particularly to patients from Sonkurai (No. 2)
Camp, where, as we understand, evacuation of all very sick patients was
practically compulsory.

2. STATE OF NUTRITION.
Apart from the state
of their disease, the nutritional state of many of the patients also
gravely prejudiced their chance of recovery. In part this was due to
poor rations at the working camps, but in part it arose from the failure
of medical officers in certain of the working camps to insist on
consumption by their sick patients of their full daily ration; in many
cases of dysentery liquid diet had been prescribed for an unconscionably
long time, resulting in practical starvation of the unfortunate patient.
Apart from the emaciation a long-standing deficiency in vitamins A, B1 &
2, and C also greatly lowered the patients power to combat their
disease.
3. EFFECTS OF JOURNEY.
The journey was made under
very arduous conditions. An inadequate supply of fit men was available
to help sick patients - food was poor and long exposure to rain storms
and severe jolting for hours were the lot of all. Under these
circumstances many patients whose fate hung in the balance had their
last chance of survival taken away from them by the strain of the
journey.
FACTORS OPERATIVE AT TANBAYA.
1. DIET.
So far from the diet being better than
at the working camps it was for a long periods considerably worse, as
will be seen from a study of the ration issues as set out in the War
Diary. Rice was in general adequate, but every other essential for a
complete diet was grossly deficient. In particular, until the bean
ration was raised from 1/3 of a bag to 1 bag on the 22nd September, the
diet contained practically no vitamin B or C. Innumerable protests and
requests for rice polishings and for more beans were made to the I. J.
A. but always met the answer that rice polishings were quite
unobtainable and that there was a great shortage of beans which were
being reserved for the camps further from the railhead. In this
connection it is interesting to note that when on October 10th we learnt
that the "A" Camp Hospital Camp. 5 kilos away, had been receiving an
adequacy of beans since its formation in July, and pointed this fact out
to the I. J. A. Camp Commandant he raised the bean issue from 1 bag to 2
1/2 bags forthwith. It is also interesting to note that from October
26th onwards regular issues of rice polishings were made available to
the camp. Had these two steps been taken earlier in the camp's history
it is my considered opinion that upwards of 100 lives would have been
saved. The deficiency in vitamins A and C undoubtedly produced a marked
lowering in the resistance of tissues to infection, thereby increasing
the frequency and severity of ulcers, furuncles, impetigo, pemphigus and
other cutaneous infections. The deficiency in protein produced a
lowering of general vitality as also did the deficiency in calcium.
2. DRUG SHORTAGES.
Until 5th November no drugs
were received from the I. J.A and even then the supply was pitifully
small and inadequate. In particular no specific therapy was available
for the treatment of Amoebic of Bacillary Dysentery, the major killing
diseases in the camp. There was no Iodoform or other drug suitable for
local treatment of the numerous tropical ulcers. No sulphur (a common,
cheap and easily procurable product) was available to treat scabies
until 5th November by which time the whole camp was infected with much
secondary suppuration and ulcer formations. Dressings were also woefully
deficient and many mosquito nets had to be sacrificed to dress the
enormous ulcers. No Iron was available to build up the anaemic patients,
and no concentrated B1 was available for the numerous severe Beri Beri
cases.
3. MALARIA.
Tanbaya was an area where Malaria of
a particularly severe type was hyperendemic. 87 deaths are shown as
being due either wholly or partially to Malaria, but beyond this the
disease had a debilitating effect throughout the camp where its
incidence reached approximately 100%. In particular Malaria caused
marked deterioration in the condition of patients suffering from ulcers
or dysentery.
SYSTEM OF ADMINISTRATION:
The system of
administration adopted at Tanbaya differed in several respects from that
customary in military hospitals. In part these differences were dictated
by local necessity, in part they were devised as possible improvements.
Lt. Col. Hutchinson as Administrative Commandant of the camp was
responsible for such services as cooking, securing of wood and water,
hygiene and pay; Major Hunt, as O C Hospital, was responsible for all
medical treatment and for the administrative control of all medical
personnel whether professional or amateur and of all patients. This
sub-division of authority worked very smoothly, and I should like here
to pay my tribute to Lt. Col. Hutchinson's loyalty, to this unfailing
tact, and to his untiring efforts in the interests of patients and of
the camp as a whole.
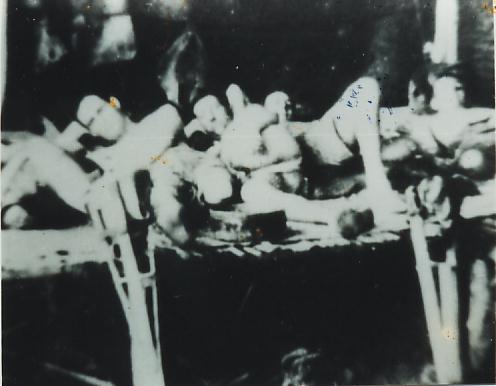
Details of medical administration were as follows:-
Patients were segregated so far, as was possible according to
their complaints; this facilitated treatment and prevented much cross
infection. Thus, one ward was devoted solely to dysentery, one ward to
pure dysentery and ulcers combined with dysentery. Two wards to ulcers
and three wards to general medical diseases, chiefly Malaria and Beri
Beri. Each ward contained in the early stages approximately 190 patients
and was under control of a Wardmaster. The Wardmaster was a combatant
officer, usually of Company Commander status or above, he had as
assistants; an assistant Wardmaster, usually a subaltern, 2 N. C. O's
who acted as C.S.M. and C.Q.M.S. respectively and a clerk. The
Wardmaster was responsible for nominal rolls, for discipline, for hut
cleanliness, for messing, for canteen supplies and in general for
everything which took place in the ward except such matters as involved
technical medical knowledge or skill. He had in addition, through the
medical officer or senior nursing N.C.O. supervisory control over the
activities of the nursing orderlies in regard to their non-technical
functions.
His system of Wardmaster control, first devised in Shimo Sonkurai Camp and further extended in Burma, proved of the greatest possible assistance in running the hospital. Discipline and general ward efficiency were better than they usually are under N. C. O. control. In particular messing functioned much more efficiently and with less complaint than is usually the case. I was particularly fortunate in having a very able body of Wardmasters; they worked, ate and slept in their wards and were completely devoted to their duties and to the interests of their patients. I should like here to express my appreciation of their valuable services.
Wardmasters were (in numerical order of their wards) Lt. I. Perry
(2/1 Heavy Bty A.I.F.), Capt. H. Walker (2/26 Bn A.I.F.). Major R.
Hodgkinson (R.A.S.C.), Major W. Auld ( M.A.O.C.), Capt. B. Berry (2/10
Fd. Rgt. A.I.F.), Capt. G. W. Gwynne (4 M.G. Btn A.I.F.), and Lt. Col.
Ferguson (18 Div H.Q.)
A Wardmasters conference, attended also by O. C. hospital,
Registrar and Messing Officer, was held at 1530 daily, and this proved a
most satisfactory means of keeping the wards in close touch with camp
policy.
In view of the shortage of drugs, all drug requisitions were
checked and countersigned by O. C. Hospital before completion. This took
place daily at 1500 hours and permitted a just distribution of drugs
between various wards and also of the conservation of necessary
supplies.
As patients in the wards improved and became fit for camp duties,
they were sent to the "labour exchange" where they were vetted by the O.
C. Hospital and then assigned to various sections of the hospital
according to the requirements of the different departments.
STAFF:
Although the number of
R.A.M.C. and A. A. M. C. personnel at Tanbaya was at its highest 142,
very many of these men arrived as patients and either died at Tanbaya or
remained as patients throughout their stay in Burma. Nine members of the
R.A.M.C. and 8 members of the A.A.M.C. died at Tanbaya, and five
R.A.M.C. and 9 A.A.M.C. were left behind as seriously ill patients when
the bulk of the camp moved in November. The maximum number of Medical
Corps personnel available for duty at any one time was 62, but the
number generally varied between 40 and 50. Under these circumstances it
was necessary for the greater part of the nursing work to be done by
volunteers from non-medical units, and the steadfast devotion to duty of
these men under circumstances of much difficulty and discomfort is
worthy of the highest praise. Many of the volunteers showed a marked
aptitude for the more technical branches of nursing and in some cases
were as good as, if not better than, the majority of the professionals.
DISEASE:
Four diseases
dominated the clinical picture. These were in the order of mortality
which they produced, Dysentery, Tropical Ulcers, Beri Beri and Malaria.
1. DYSENTERY.
In the absence of
facilities for bacteriological or sigmoidescopic examination it was
impossible in most cases to differentiate between Amoebic and Bacillary
Dysentery. Clinically however, I formed the opinion that the former
disease predominated, and autopsy and the result of treatment of five
cases by Emetine in November (this was all the Emetine we ever received0
tended to confirm this impression. The dysentery wards were amongst the
most tragic places in the camp. Many of the patients put up a gallant
struggle forcing their rice down day after day and week after week in a
heroic effort to stay alive until adequate facilities for treatment
arrived. Dysentery alone caused 114 deaths, and in association with
other diseases played a part in killing 334 men. In many cases an attack
or recurrence of Dysentery was the terminal factor in carrying off
patients suffering from Beri Beri or Ulcers.

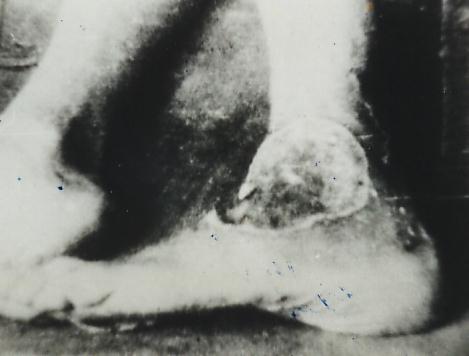
2. TROPICAL ULCERS.
These were
of very great frequency and inmany cases of horrifying severity. Huge
areas of skin, flesh and in some cases bone were eaten away and the skin
appeared to posses little or no resistance to the infecting organisms.
Ulcers followed small scratches or cuts with distressing frequency and
not a few patients died of Ulcers which actually developed in the camp.
Capt. F. J. Cahill was in charge of the Ulcer Wards throughout, and has
prepared a detailed memorandum on the subject of these ulcers. The lower
extremity, and in particular the region of the Tibia was the site of
election for the formation of ulcers. they could, and did however occur
in almost any area of the body, as for example over the great
trochanter, over the lower spine, in the groin, over the scapulars, on
the elbows, wrists and fingers. A few cases responded strikingly to the
application of Sulphanilamide or Iodoform, and had these drugs been
available in anything like adequate amounts much life would have been
saved. In the absence of these drugs simple cleansing with Eusol or
Saline two or three times daily provided the best results, which however
in many cases were disappointing. Amputations were performed in 60 cases
(for details see Capt. Cahill's memorandum), but here also the results
were in general disappointing, owing to the poor general condition of
the patients and the frequent occurrence of severe secondary sepsis in
the stump. It was noticeable that an attack of Dysentery or Malaria
caused considerable deterioration in the condition of the ulcer which
hitherto had progressed quite favourably. Ninety two patients died of
ulcers alone and 105 of ulcers complicated by other diseases.
3. BERI BERI.
Beri Beri was
widespread through the camp, and at one time there was upwards of 600
patients showing clinical manifestations of the disease. It was also
more severe than any which I had previously sen, the oedematous and
cardiac types predominated. A further complication which caused much
loss of life in Beri Beri cases was the frequency with which grossly
oedematous Beri Beri patients developed a rapidly spreading gangrene in
their water logged extremities. This complication was almost invariably
fatal. Many patients remained oedematous for several weeks and in such
cases cardiac deterioration generally occurred or followed on the
oedema. Cardiac Beri Beri was both common and severe. Practically every
clinical cardiac abnormality ever recorded in Cardiac Beri Beri was
observed at Tanbaya. Hearts were enlarged both to the right and to the
left, chiefly the latter. The rate varied both upwards and downwards,
bradycardia was very common. Abnormalities of rhythm were relatively
frequent. These generally took the form of extra-systoles, although
auricular fibrillation was observed on a number of occasions, frequently
just before death. Variations in pulse volume were not infrequent and
generally of poor prognostic significance. Abnormalities in heart sounds
were frequent. A splitting of the first sound was the most
characteristic change. Systolic murmers occurred frequently. Gallop
rhythm was noted sometimes. Thee pulmonary secondary sound was
frequently loud and banding. Cyanosia and other sounds of congestive
heart failure were relatively infrequent. Sudden death occurring in the
middle of the night was not uncommon. Administration of Vitamin B1
intravenously saved a certain number of lives when cardiac emergencies
occurred, but of this, as of all other valuable drugs, supplies were
grossly inadequate. 68 patients died of Beri beri alone and in a further
260 cases Beri Beri was one of the causes of death.
4. MALARIA.
Malaria was
practically universal throughout the camp, and in August and September
relapses were very frequent, as owing to the shortage of supplies it was
not possible to give quinine treatment for longer than 7 days. After the
end of September supplies increased considerably, and it was possible to
increase the course from 24 grs. daily for 7 days to 32 grs. daily for
12 days, accompanying the latter with .02 grs. Plasmoquin daily. After
this step was taken there was a marked fall in the incidence of malarial
relapses. Microscopic examination conducted by the I. J. A. showed a
relatively frequency of B. T. and M. T. infection of approximately 2 to
1.
One of the outstanding clinical features of the Malaria at Tanbaya
was the high degree of resistance to quinine. In many cases of undoubted
malaria, the fever did not come under control until 6, 7 or 8 days after
treatment had commenced. A number of patients were observed to relapse
on the 10th or 11th day of treatment whilst still taking 32 grs. of
quinine daily. Finally, every person who had hitherto been protected
from Malaria in Thailand by suppressive Atebrin had clinical Malaria in
Burma although continuing to take Atebrin regularly. Ten people were
thus affected. Cerebral Malaria occurred in about 30 cases, many of
which responded satisfactorily to parenteral quinine. Haemoglobinuria
was seen half a dozen times but no true case of black water fever
occurred.
5. TYPHUS.
A 14 day fever
clinically resembling typhus in many respects was observed in about 40
cases. No rash and no eschar were seen, but previous experience of this
disease left me in little doubt as to the nature of the fever.
Serological confirmation of the diagnosis was of course impossible. The
typhus in general was relatively mild and only two or three cases
succumbed.
6. CATARRHAL JAUNDICE.
About 50
cases of this disease were seen, all mild and none fatal.
7. RESPIRATORY DISEASES.
Coryzas were frequent, but only about half a dozen pneumonias were seen,
two of which were followed by empyaema.
8. SCABIES.
Scabies spread
steadily from the formation of the camp onwards, and by November when
the supplies of sulphur arrived it was almost universal. Scabies had of
course a high nuisance value, but in addition to this it gave rise to
much secondary infection, and in some cases to severe ulcers which
resulted fatally. Treatment was instituted immediately on the arrival of
the sulphur in early November (coking oil being used as a base). Much
improvement naturally occurred in the scabies but the sulphur came too
late.
RECORDS.
The register of deaths
is contained in the War Diary. The camp roll contains an entry of the
diseases from which the various patients suffered during their stay at
Tanbaya. With view to giving such patients some individual record of his
illnesses, entries signed by medical officers were made in both British
and Australian pay books. Where pay books had been lost, cards or bamboo
slips were issued on which the appropriate particulars were inscribed.
Every man who left Tanbaya should have with him a full record of the
illnesses from which he suffered in that camp.
EVACUATION.
As early as
September strong representations were made to the I.J.A. that many
hundreds of patients would not successfully survive a long railway
journey (see the letters from Major Hunt quoted in extense in the War
Diary). As a result of these representations considerable leniency was
allowed in the selection of patients to travel. Much care was taken with
this selection and as a result, of the 900 patients who left Tanbaya for
Kan Chan Buri only two failed to survive the arduous 5 to 6 days
journey.
A staff of 102 was left behind in Burma to look
after 218 patients. Of these patients approximately 85 were suffering
from Dysentery and approximately 65 from Ulcers; the majority of the
remainder had beri beri. If conditions prevailing in November persist,
and if the patients are evacuated in February as seems probable, I
anticipate a mortality of 90/100. This would include about 60 dysentery
cases, about 15 ulcer cases, and about 15 beri beri cases.
CONCLUSION.
The Burma
Hospital Camp for reasons stated above, could not be regarded as a
success. Its partial failure however was much mitigated by the work of
the administrative staff, by the devotion to duty of the wardmasters and
by the professional skill and knowledge displayed by some of the medical
staff. In this connection I would particularly mention Major W. J. E.
Phillips (R.A.M.C.), Capt. Emery (R. A. m. C.), Capt. F. J. Cahill (A.
A. M. C.), and Assistant Surgeon Wolfe (I. M. D.). Outstanding nursing
work was performed by Sgt. G. Nichol (A. A. M. C.). and by Cpl. Skippen
and Cpl. Sutton (R. A. M. C.)
KANCHANABRI
(Sgd) Bruce Hunt. Major A.A.M.C.
23.12.43
Commanding Burma Hospital
Visitors
This website was created using Microsoft Expression Web 4 © 2008-12